

During a game of Napoleon in Egypt, the French Player has the opportunity, through scientific research, to build a “military hospital”. This precious asset will greatly increase the durability of the French troops. In this article, we’ll look at the historical aspect of this element, before considering the game mechanics around it in a follow-up article.
Desgenettes and Larrey were two French military physicians who followed Bonaparte from the Italian campaign (1796) to Waterloo (1815). The medical breakthroughs of the Egyptian expedition are largely thanks to these two dominating figures. René-Nicolas Dufriche Desgenettes was chief physician, and Dominique-Jean Larrey was chief surgeon. Both displayed remarkable skills in organizing the Medical Corps in Egypt. In a difficult geographical, climatic and epidemiological context, they were crucial in the emergence of modern military medicine and played a full part in the expedition’s scientific achievements.

For these two doctors, the expedition was a real challenge. The Medical Corps consisted of 168 medical officers, more than half of them surgeons, who had to ensure the good health of some 30,000 men. It’s worth remembering that, in those days, a surgeon was a practitioner with basic training in charge of external and traumatic ailments, while a doctor was a specialist who studied longer to be able to treat the more complex “internal diseases”. They were assisted by “nurses” in very short supply, who were actually soldiers placed at their disposal or men recruited locally from the Coptic or Armenian populations.
Despite this manpower shortage, the remoteness, the unknown illnesses and the loss of much of their equipment during the disastrous Aboukir battle, Desgenettes and Larrey’s dedication enabled them to achieve incredible results. Of the nearly 9,000 men who lost their lives during the expedition, less than half succumbed to disease – a much lower rate than what was typical before the 20th century. Of these losses due to disease, around 1,700 (30%) victims died of the plague. Speaking of the plague, 54 medical officers died of it, making it the leading cause of death for doctors and surgeons in Egypt. This is partially explained by the fact that the medical staff often locked themselves in the lazarettos to care for the sick and avoid contagion, a heroic act given the high risk of contamination. In the end, 82 members of the medical staff perished, i.e. 49% of the workforce, while troop losses amounted to 30%.
Most of the wounded were initially treated in the same way as on all other battlefields of the time: after the battle. Limb injuries were handled, while wounds to the skull, thorax or abdomen were off-limits. Whether wounds were caused by bladed weapons, bullets or cannonballs, the high risk of post-operative infection meant that amputation was the preferred treatment. French surgeons were impressed by the depth of the wounds inflicted by the fearsome oriental sabers of the Mamluks. Right from the start of the campaign, in addition to heat-related incidents, doctors and surgeons were struck by the frequency of ophthalmic ailments due to the sand and the sunny weather. The lack of fresh fruit and vegetables also led to cases of scurvy, and many ailments were caused by poor water quality. Dysentery was common as were all sorts of “fevers”, a catch-all since practitioners at the time could not distinguish between viral diseases, malaria and typhoid.

The plague was already present in Egypt when the French arrived and killed many in the garrisons of Alexandria and Damietta. It also accompanied the army from El Arish to Saint Jean d’Acre, via Gaza and Jaffa. There was an odd theory running around at the time that only those afraid of the disease contracted it. This may partly explain Bonaparte’s visit to the Jaffa lazaretto. Desgenettes also reported that on several occasions, Bonaparte and other generals grabbed sick people to help transport them. Contamination inside the lazarettos was caused by rat fleas but doctors of the time had no such knowledge and instead believed that the air quality was the cause of the plague’s proliferation. Hence the ill-advised confinement of plague victims and their doctors in quarantined lazarettos.

Faced with the many illnesses that the torrid climate, temporary bivouacs and lack of drinking water were causing in the army, Desgenettes introduced rigorous hygiene and prophylactic measures: body washing, clothes cleaning, premises disinfection and food intake monitoring. The structuring of the health service involved the creation of numerous military hospitals throughout the occupied country, with coordinated and permanent exchanges of information and instructions. Meanwhile, similar civilian hospices were created and managed, as Bonaparte was keen to ensure that the expedition appeared in a positive light to the native people.
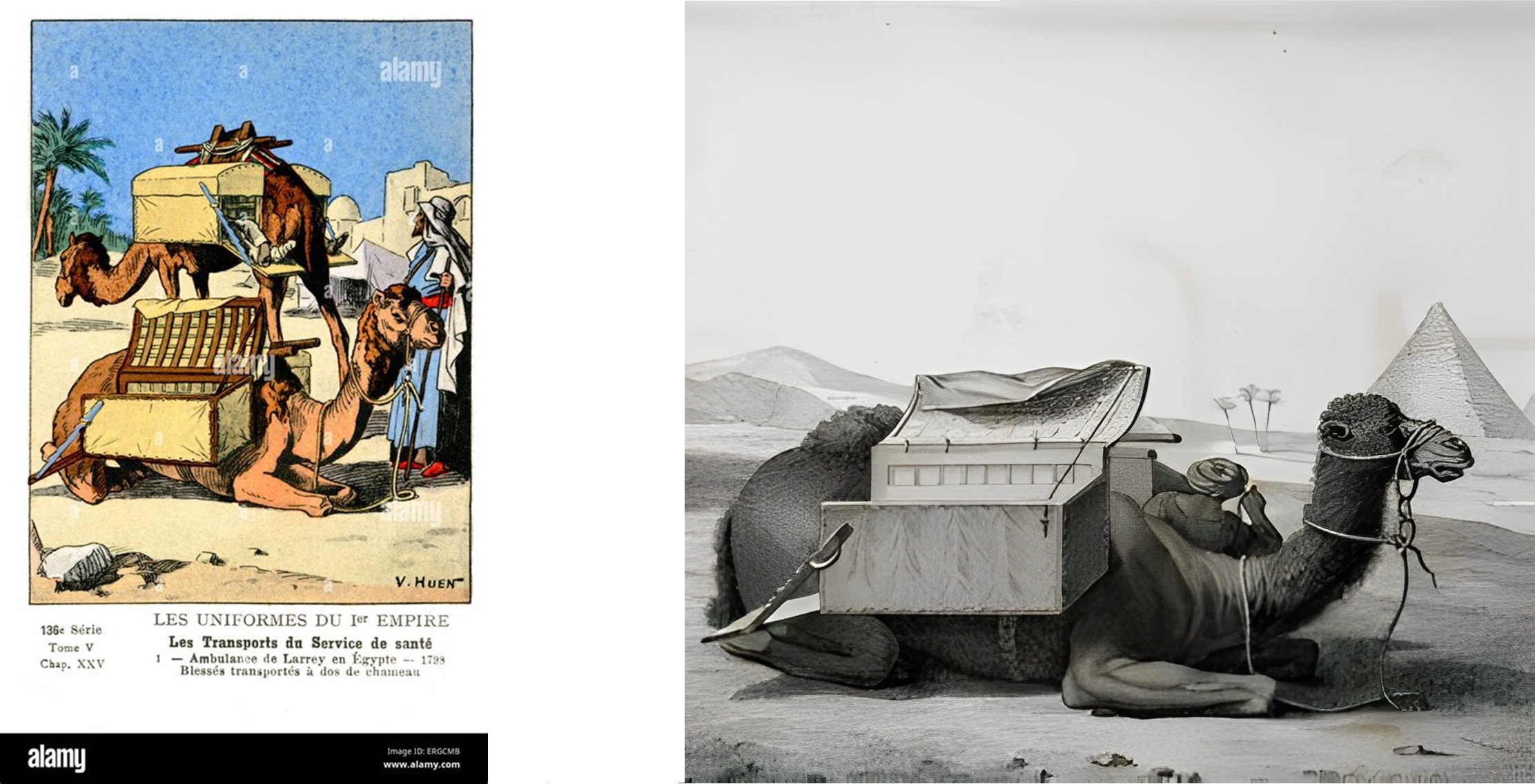
Larrey was noticed by Bonaparte during the siege of Toulon (1793), and pretty much never left his side thereafter. He was an innovator on the battlefield. He defied the ban on medical officers staying within three miles of the fighting and waiting until the battle is over to help the wounded. Inspired by the speed with which mounted artillery batteries moved, he designed “flying ambulances” capable of rescuing soldiers right into the heat of battle. In Egypt, faced with a shortage of horses and adapting to local conditions, the surgeon set up his flying ambulances on the back of dromedaries.
“I had one hundred baskets built, two per dromedary, arranged in the shape of a cradle that the animal carried on each side of its hump, suspended by elastic straps by means of a rocking extension: they could carry a wounded man lying down in its entire length.”
For Larrey, the surgeon had to operate as close to the front as possible: time was of the essence. Surgery success required speed of intervention, tactile precision and judgment of what was necessary: it therefore relied first and foremost on experience. This was a more humane way to save the greatest number of wounded at a time when there is no anesthesia, no asepsis or antisepsis, and no transfusion. Larrey is the father of urgent care! When Bonaparte left (August 23, 1799), the surgeon stayed behind until the French defeat and kept caring for the sick and wounded, founding a school of surgery and a school of medicine, both open to the natives. He embalmed Kléber, assassinated in Cairo on June 14, 1800, as well as his assassin!
The overriding feeling when attempting to draw a conclusion to this military and sanitary expedition is, first and foremost, the impression of witnessing the birth of a modern health service, made necessary by the spatial and temporal constraints surrounding the expedition. Isolation following the Aboukir disaster, the absence of any real prior medical presence on site, the pressure of combat and new pathologies in an unfamiliar environment all contributed to this structuring. The strong, lasting bond between the three protagonists (Bonaparte, Desgenettes and Larrey), which goes back to their participation in the Italian campaign, also played a considerable role. The General-in-Chief’s esteem for the two practitioners never wavered and in return, the dedication of both men was unfailing. Truth is, the logistics were remarkable: hospitals opened as needed and communicated with each other, all under precarious conditions and with marked hostility from the population on many occasions. A real esprit de corps set in over the months. Did the Egyptian campaign change military medicine? One thing’s for sure: this expedition was undoubtedly the start of the revolutions introduced by Larrey during further Napoleonic campaigns, completely reimagining the perspective of care on the battlefield with speed, audacity and proximity.
Previous Napoleon in Egypt InsideGMT Articles


Author: Pascal Toupy
